Catheter ablation of arrhythmias
1.1 Catheter Ablation
Miller & Zipes, (2002) describes briefly the process of cardiac ablation, the risks of the operation, the post-processing phenomena and the target group which needs this kind of cardiac surgery. The Catheter Ablation (CA) is used to treat a variaty of arrhythmia such as atrial tachycardias (AT) or supraventricular and ventricular tachycardias (VT). The selection of CA operation is determined after the evaluation of the patient’s risks and benefits of his tachycardia characteristics by the medical doctors. The majority of patients with VT after a heart attack or cardiomyopathy have a high risk of mortality (Miller & Zipes, 2002).
1.2 Mechanisms of Catheter Ablation
When a CA has decided the electrophysiology doctor starts an episode of tachycardia to determine the specific characteristics of it. The patient stops his meditation for a period before the operation. A 3D mapping system, a fluoroscopy used for the navigation of the catheter inside the vascular system of the ailing. The electrical activity of the patient is monitoring by the catheter inside the heart in the region of interest (ventricle or atrium mainly). A sequence of ablation is planning concerning the reentry paths of the specific cardiac region. (Miller & Zipes, 2002
1.3 Ventricular Tachycardia Arrhythmias
There are many kind of VT like monomorphic, pleomorphic, polymorphic and multiply monomorphic (Table 1) related to the variation of the configuration of the QRS complex of the electrocardiogram occurring during the same episode of VT ((Aliot et al., 2009)). The VT are classified in structural and non-structural disease. The main mechanisms of tachycardias with structural heart disease is the scar-related reentry. In this myocardial scars there are reentry phenomena owing to the continue excitation of the same paths. Reentry usually occurs via muscle bundles which is steel alive after a myocardium infarction (MI). Approximately the 5% of all SMVTs is caused by reentry within the Purkinje system (Aliot et al., 2009).
| Table 1: Clinical Morphologies of Ventricular Tachycardias (VT) (reproduced from Aliot et al., 2009) |
|---|
| Monomorphic VT : has a similar QRS configuration. Nevertheless, variability in initial QRS morphology may be observed, followed by stabilization of QRS complex. |
| Multiple monomorphic VTs : relates to a variety of monomorphic VT occurring at different times and episodes. |
| Polymorphic VT : has a continuously changing QRS configuration for each cardiac cycle, displaying a modified ventricular activation. |
| Pleomorphic VT : has a variety of QRS complex occurring during the same episode of VT, but the QRS is not continuously changing |
| Right and left bundle branch block-like—VT configurations : terms used to describe the dominant deflection in V1, with a dominant R-wave described as ‘right bundle branch block-like’ and a dominant S-wave as ‘left bundle branch block-like’ configurations. |
| Unmappable VT : the examination of multiple sites to define the activation sequence or perform entrainment mapping is not feasible, owing to hemodynamic intolerance that necessitates immediate VT termination. |
| Ventricular flutter : is a term defines by a rapid VT with sinusoidal QRS configuration that makes tricky the identification of the QRS morphology. |
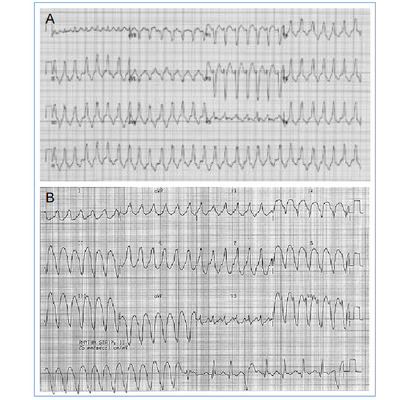
| Figure 2: Clinical morphologies of VT |
|---|
{kind=link}
Contributors
Michail Mamalakis
Phd student, computational modeling of cardiac electrophysiology,
University of Sheffield, Computer Science Department